Category: Healthcare and public health research

The way to build bridges instead of walls is still long.
The way to build bridges instead of walls is still long, but I am happy to have got European Union funding for this project. Africlinique project aims to increase the
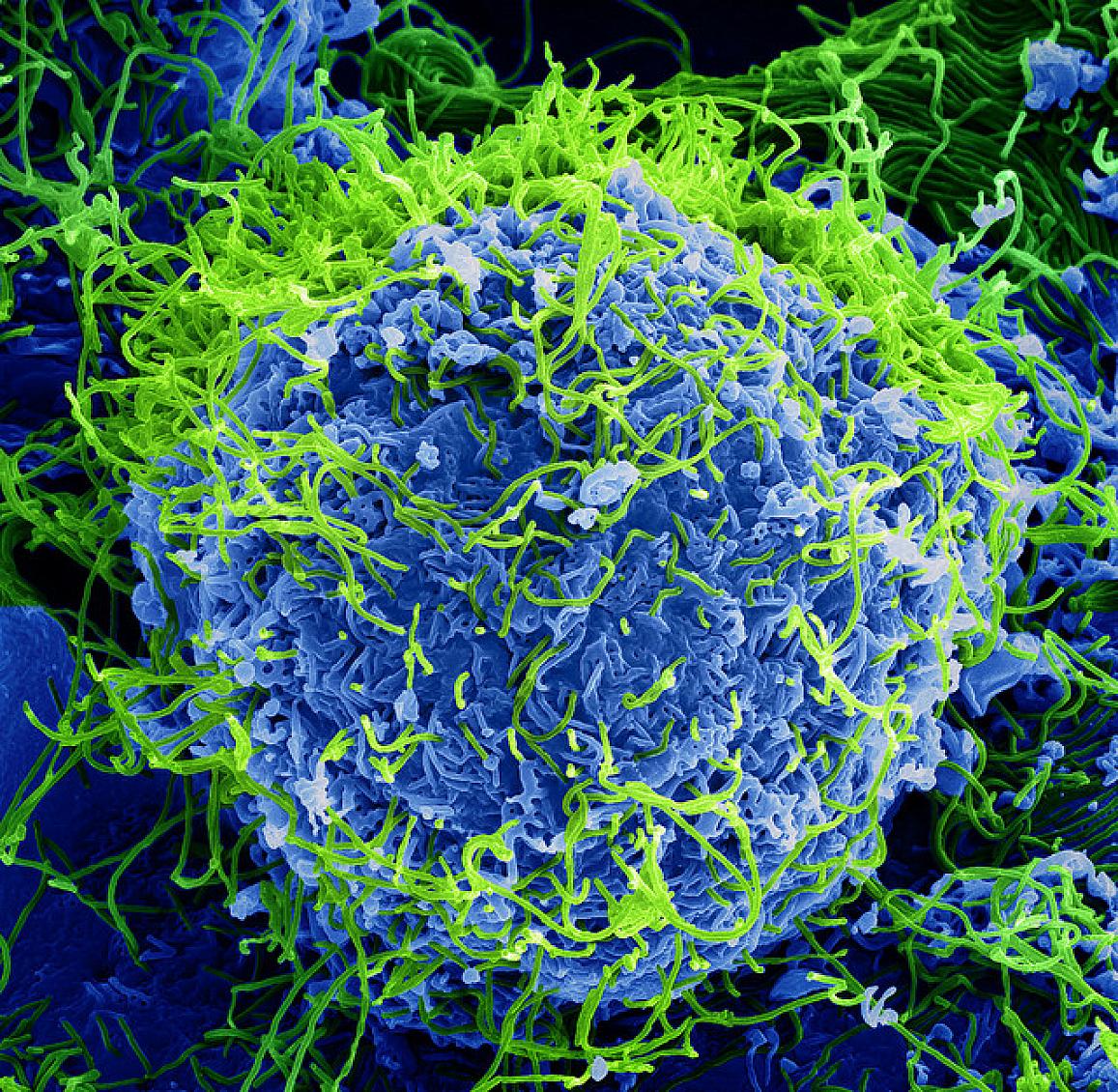
Ebola vaccines at a la glance

Ebola vaccine candidates are currently being evaluated in phase I–III clinical trials conducted in Africa, the EU and the US. Although preclinical development of candidate vaccines utilise different platforms, including
Controlled Human Infection Model (CHIM) studies

In a Controlled Human Infection Model (CHIM) study, a well-characterised strain of an infectious agent is given to carefully selected adult volunteers in order to better understand human diseases, how they spread, and
Ebola outbreak in Republic Democratic of the Congo: switching from MEURI (Monitored Emergency Use of Unregistered and Investigational Interventions) to a RCT (Randomized Clinical Trial) for 4 experimental medications in the treatment of Ebola Virus Disease
An international research team has begun patient enrollment in a clinical trial testing multiple investigational Ebola therapies in the Democratic Republic of the Congo (DRC). The randomized, controlled trial is